The best screening test is the one that gets followed up on
Gastroenterology
The Best Screening Test is the One That Gets Followed-up on
Caravaggio — The Incredulity of Saint Thomas (1601) Sanssouci Picture Gallery · Potsdam Thomas presses his finger into the wound to verify what he doubts — not out of defiance, but out of the need to know. A meditation on empirical conviction: belief deferred until the evidence is personally confirmed.
The Problem
Colorectal cancer screening saves lives – but only when the process is completed. The well-known saying by Dr. Sidney Winawer, “the best test is the test that gets done and done well,” has driven campaigns to boost screening uptake. Yet a critical gap persists: nearly half of patients with a positive stool-based test never complete the follow-up colonoscopy. Without that diagnostic step, screening delivers zero benefit – and patients bear only the costs and harms.
The Approach
Using the MISCAN-Colon microsimulation model, we simulated 10 million individuals offered a one-time FIT screening at age 45. We systematically varied both screening adherence and follow-up colonoscopy adherence across five levels (0%, 25%, 50%, 75%, 100%) to quantify how each step of the pipeline contributes to life years gained. We complemented the modeling exercise with a comprehensive review of clinical evidence and system-level barriers.
What We Found
The simulation demonstrated that follow-up adherence is at least as important as screening adherence. Scenarios with 0% follow-up yielded no life years gained compared to no screening at all – even with 100% screening uptake. Remarkably, 25% screening with 75% follow-up produced similar benefits to 75% screening with 25% follow-up. In safety-net health systems, where follow-up rates fall below 45%, even blood-based screening tests were not cost-effective compared to no screening.
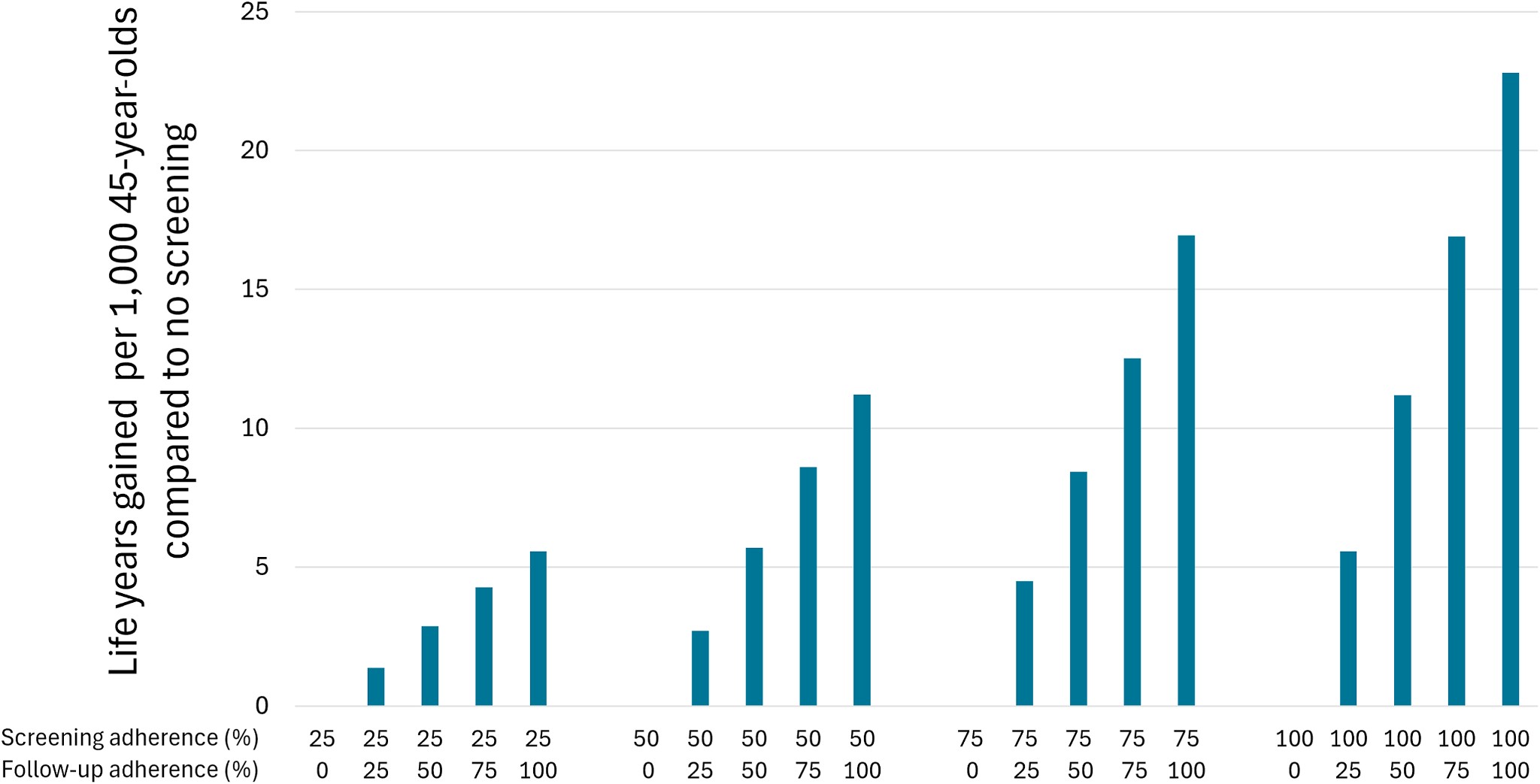 Life years gained per 1,000 screened at age 45 (FIT vs no screening), across screening and follow-up adherence levels.
Life years gained per 1,000 screened at age 45 (FIT vs no screening), across screening and follow-up adherence levels.
Why It Matters
The CRC screening pipeline is leaking. Without timely follow-up colonoscopies, even perfect screening uptake and high-quality tests deliver no benefit. System-level interventions – patient navigation, reminder systems, care coordination, and rideshare programs – are essential to close the gap. As NCQA develops new HEDIS measures for follow-up adherence, the message must shift: screening is complete only when appropriate follow-up is provided.
Citation
van den Berg, D.M.N., Brück, C.C., Nascimento de Lima, P., Alarid-Escudero, F., Hahn, A.I., Lansdorp-Vogelaar, I., & Colorectal Working Group of the Cancer Intervention and Surveillance Modeling Network (CISNET) [incl. Roa, J.]. (2026). The best screening test is the one that gets followed up on. Gastroenterology. DOI: 10.1053/j.gastro.2026.02.013
Citation
@article{den_berg,_d.m.n.2026,
author = {den Berg, D.M.N., van and C.C. , Brück and de Lima, P.,
Nascimento and F. , Alarid-Escudero and A.I. , Hahn and I. ,
Lansdorp-Vogelaar and Working Group of CISNET {[}incl. Roa, J.{]},
Colorectal},
title = {The Best Screening Test Is the One That Gets Followed up On},
journal = {Gastroenterology},
date = {2026-02-23},
url = {https://jorgeroac.com/publications/papers/peer-reviewed/gastro-screening-followup/},
doi = {10.1053/j.gastro.2026.02.013},
langid = {en}
}